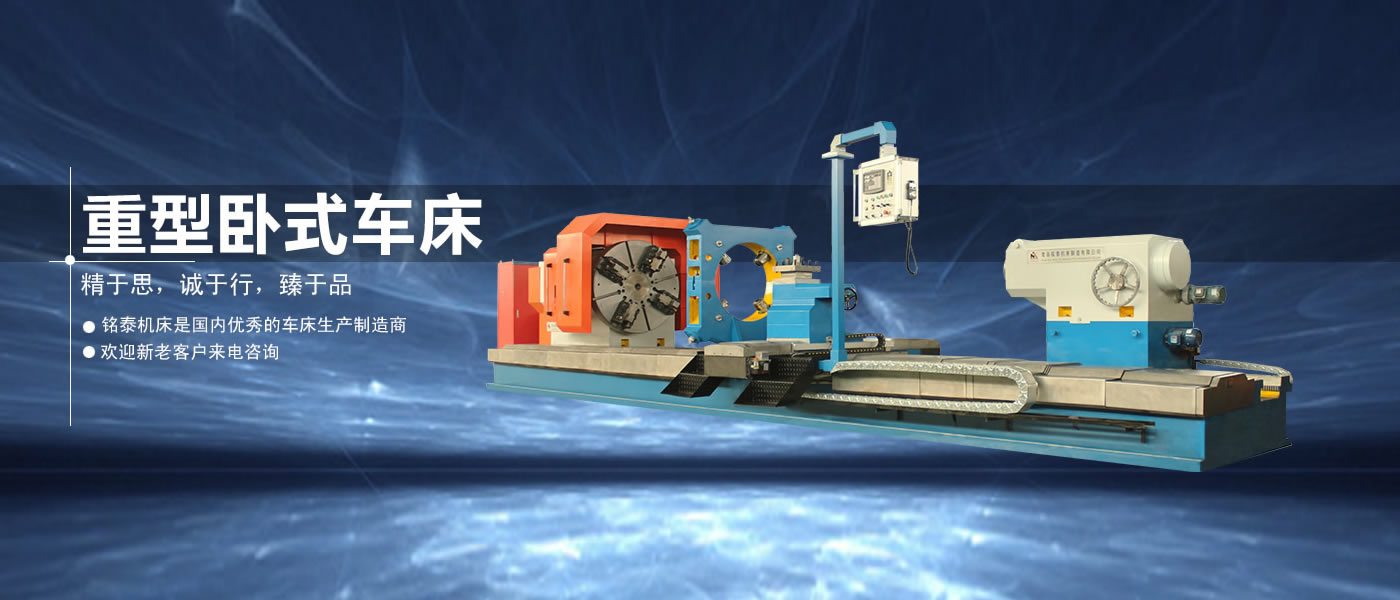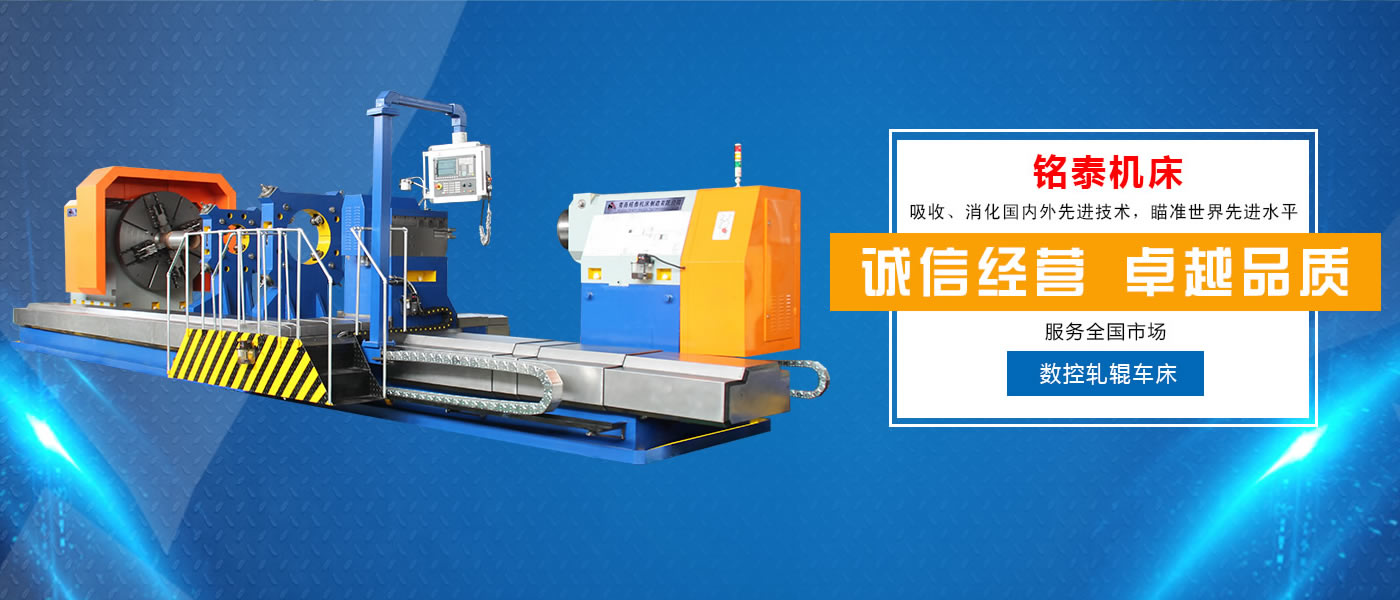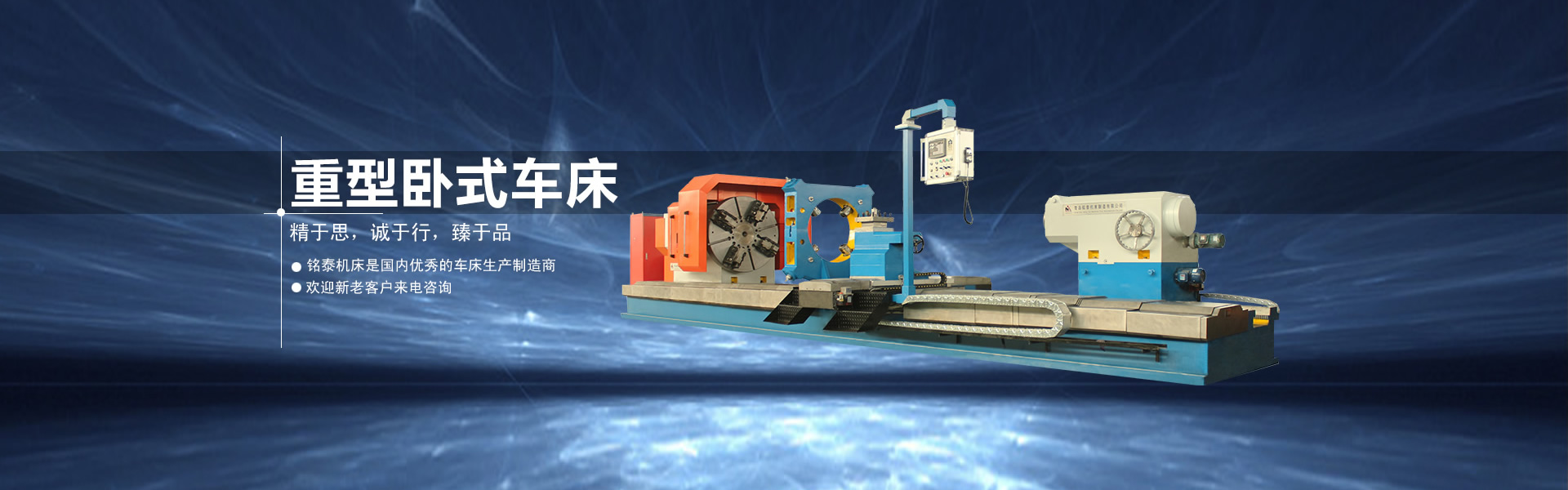
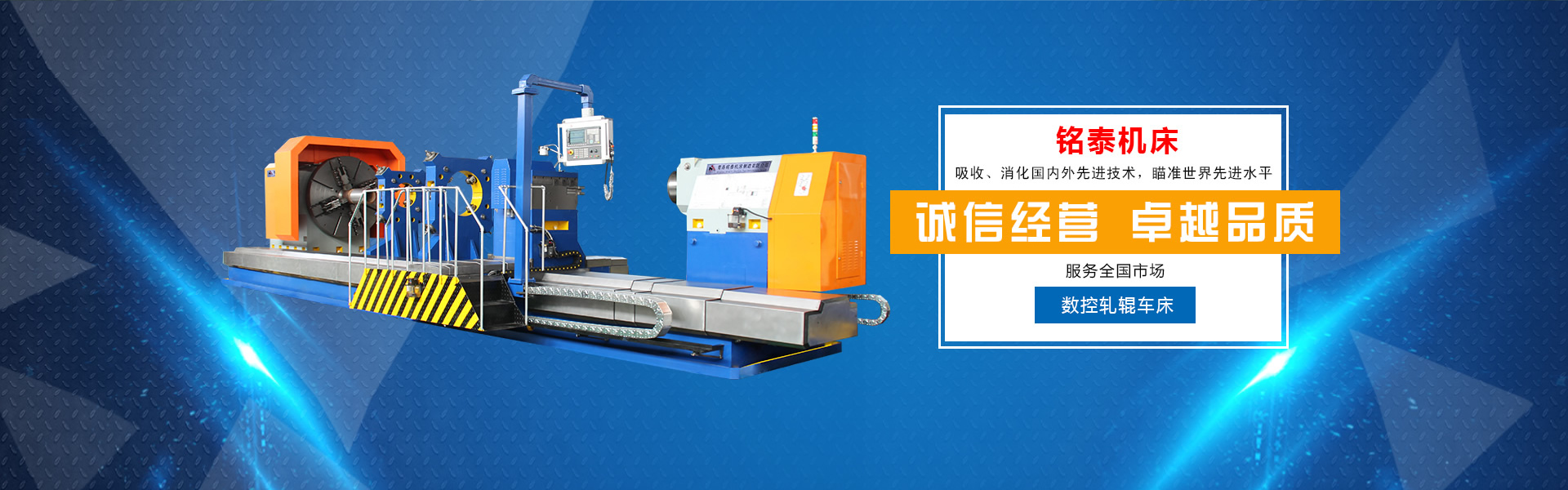

万搏线上平台是国内优秀的车床生产制造商,是一家集设计研发、生产、销售、售后服务为一体的专业生产厂家,拥有多年生产大型落地车床、大头车床、重型数控卧式车床、数控端面车床、大型立式车床、重型机床、法兰专用机床的丰富实际操作经验,铭泰机床是吸收、消化国内外先进技术,瞄准先进水平而设计开发的。公司坐落于美丽的海滨城市——青岛,位于青岛市城阳区流亭工业园,东依崂山风景名胜区,西距流亭国际机场2公里,南邻青银高速,北临济青高速出口,地理环境优越、交通便利。 主导产品有各种规格型号的大型连体、分体落地车床,重型卧式车床,立式车床等专用车床,还可根据用户特殊要求进行非标设备的设计生产。技术含量高,结构合理,钢性强,性能优越,且高效节能,多年来畅销国内各地,深受用户青睐。公司生产的系列车床主要适用于风电机械、纺织机械、矿山机械、化工机械、铸造机械、橡胶机械、轮胎模具、锅炉压力容器、各种法兰、管件、阀门及盘状类、大直径工件的切削加工,能够车削各种大型零件的内外圆柱面、圆锥面、端面及曲面圆弧等成型表面。公司本着“精于思,诚于行,臻于品”的经营理念,以“开放、科学、创新、协作”的企业精神,为客户提供卓越的机床产品。我们视产品的质量如企业的生命,放心的品质、更优质的服务,是铭泰机床对每个客户的承诺··· ...



Mingtai machine advantage
The equipment is widely used
Advanced equipment
Our commitment

扫一扫加好友